
Everyone Has Something
Whole body imaging and the fight of weak priors


This week Midjourney announced a machine that scans your entire body in about a minute. You step into a shallow pool and a platform lowers you through a ring of submerged ultrasound sensors, and a minute later there is a map of everything inside you, with no radiation and no needle involved. The pitch is early detection: finding a cancer while it is still small enough to cut out.
Midjourney is best known for making AI images from text prompts. The scanner is its first piece of hardware, and the company says it eventually wants 50,000 of them doing a billion scans a month.
Whole body scans aren’t new. Prenuvo has been selling whole body MRIs to healthy people for five years now, and a handful of competitors have followed. What kept them rare was money. A whole body MRI runs $600 to $2,000 out of pocket and insurance won’t cover it for someone with no symptoms, so the scans went mostly to people who could afford an expensive maybe. Midjourney is promising the same thing at roughly the price of a massage, and whether their particular machine works or not, cheap whole body imaging is clearly coming.
Every single person has something weird in their body. A whole body MRI of a healthy person turns up something abnormal in 80 to 97 percent of people, and almost all of it is harmless. One review of more than 6,000 screening scans found 91 percent of the findings were benign and about one percent were cancer. These machines reliably find things, and what they find is overwhelmingly noise.
Many doctors object for a statistical reason: in someone with no symptoms, cancer is rare, so most flagged findings are false alarms. Each one can lead to another scan, a specialist visit, sometimes a biopsy, and weeks or months of waiting.
What Midjourney built
The Midjourney scanner is an ultrasound device. It uses Butterfly Network’s ultrasound-on-chip, the same component in their handheld probes, arranged into a ring you pass through underwater so it images you from every angle. Midjourney licensed the technology in late 2025 . The company markets the result as “Ultrasonic CT,” which is a bit confusing, since CT means X-ray computed tomography and there are no X-rays involved, and it compares the images to MRI, which uses magnetic fields rather than sound.
By the company’s own account it’s not a diagnostic device yet. It has no FDA clearance, it currently outputs only body-composition maps of muscle and fat, and the founder, David Holz, said it doesn’t yet use any AI. The diagnostic version that would rival an MRI is a regulatory process the company says it intends to start later. The first location is a spa in San Francisco penciled in for the end of 2027, and the stated goal is 50,000 machines doing a billion scans a month, paired with a claim that enough early imaging could prevent 30 percent of deaths and half of all healthcare spending. There is no evidence I could find for that last figure.

Maybe Midjourney is the company that drives whole body imaging costs down an order of magnitude, maybe it’s a competitor, but cheap and frequent scanning is coming quickly either way.
What whole body imaging finds
Prenuvo’s argument is that the cancers that a whole body scan turns up are disproportionately the ones nothing else would have caught in time, the cancers with no routine screening test. Their Polaris study followed about a thousand mostly asymptomatic adults and found biopsy-confirmed cancer in 2.2 percent of them, most in people who felt fine, a lot of them kidney, bladder, and ovarian cancers that tend to surface late. Among the people whose scans came back clean, 99.8 percent were still cancer-free a year later.

Those numbers come from the company that sells the scan and are drawn from people healthy and motivated enough to spend a few thousand dollars checking on themselves, so they are worth treating with some caution. There is no randomized trial showing that whole body MRI makes average-risk people live longer, and no mortality data at all. Prenuvo has a 100,000-person study running to look for some, and the results are years out.
False positives and overdiagnosis
A scan finding can be bad in two different ways:
The first is an ordinary false positive. The scan flags a spot, the spot looks like it could be something, you do more tests, and it turns out to be nothing. The information was wrong, and the cost was the workup it took to find that out and the anxiety in the meantime.
The second is overdiagnosis, which is stranger. The scan finds a real cancer and the biopsy confirms it, so the test was not a false positive. But sometimes that cancer was never going to hurt you. It would have sat there doing nothing for the rest of your life while you died of something else decades later. Because the scan found it, it gets treated, and you absorb the surgery, the radiation, and the years of follow-up scans.
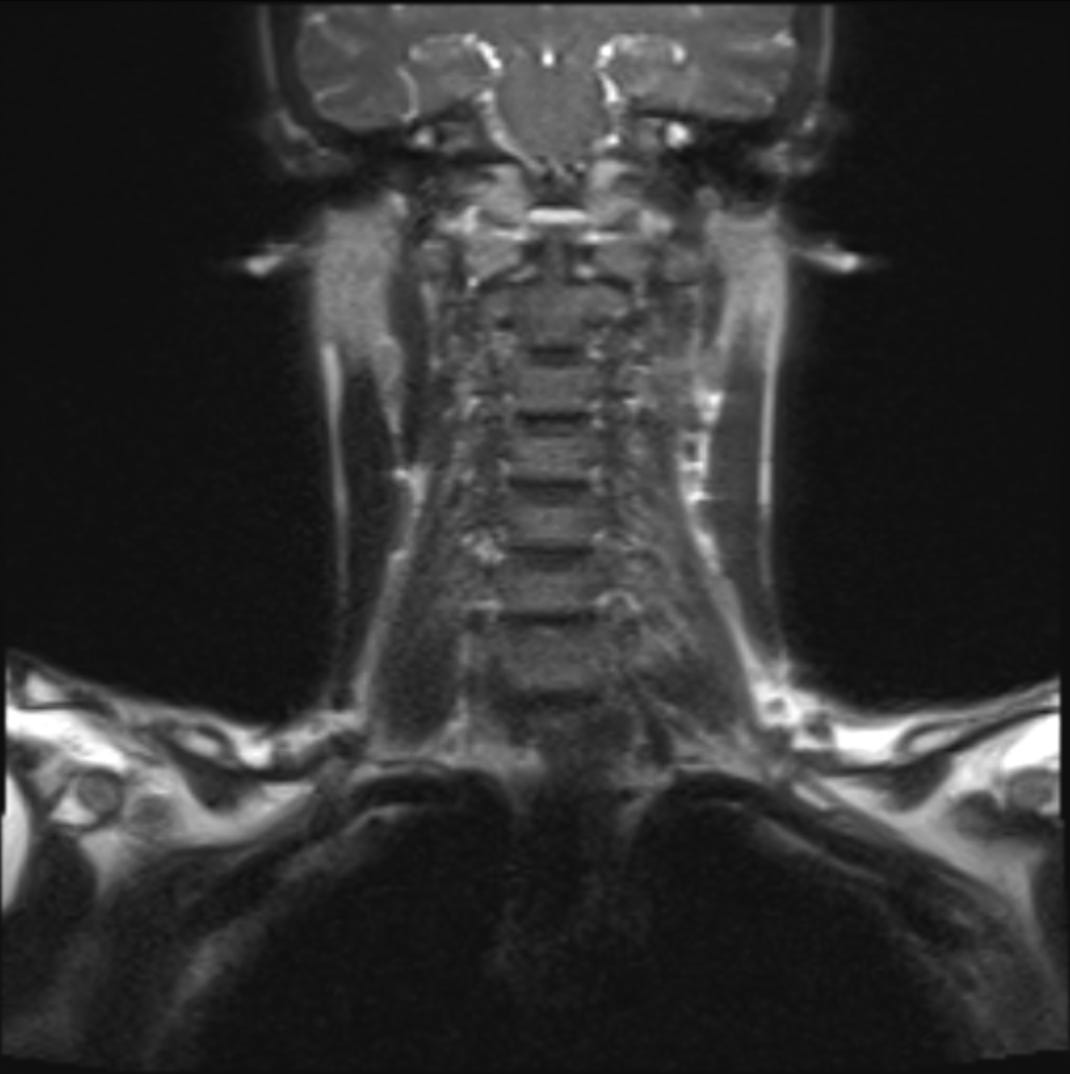
Thyroid cancer is the textbook example. As neck imaging became common, thyroid cancer diagnoses climbed steeply across dozens of countries while the death rate stayed flat. A 2024 analysis put the share of thyroid cancers diagnosed worldwide that were overdiagnoses at roughly three in four.
The hard thing about overdiagnosis is that accuracy does not solve it. The test wasn’t inaccurate and the cancer was really there. The issue comes from the health system you’re in treating every cancer it finds as urgent, including the fraction that would have done nothing if left alone.
The exception
There is one group of people for whom whole body MRI is not controversial at all. People born with a broken copy of the TP53 gene have Li-Fraumeni syndrome, which gives them an extraordinarily high lifetime risk of cancer, often several cancers, often young. For them an annual whole body MRI is recommended by the NCCN as standard care. A baseline scan finds a new cancer in about 7 percent of TP53 carriers, almost always early enough to treat, and surveillance meaningfully improves how long they live.
It produces the same flood of incidental findings, and it false-alarms about 40 percent of the time even in this group, and it is still clearly worth doing for them. The difference is the prior: in a TP53 carrier, a suspicious finding is much more likely to be real cancer.
Priors
This tradeoff is older than whole body imaging. It shows up in every screening test, and it turns on the prior: the chance the person had the disease before you ran the test at all.
Take a test that performs relatively well, one that catches a real cancer 90 percent of the time and falsely flags a healthy person only 9 percent of the time. Run it on 10,000 people in a population where one in a hundred actually has the cancer. A hundred people have it and the test catches 90 of them. Among the 9,900 who are healthy, a 9 percent false-alarm rate produces about 890 positives. So out of roughly 980 people who get a positive result, only 90 have cancer. The test worked exactly as designed, and a positive result still means the person is probably fine, because there were so few real cancers in the population to begin with.
Being one of those 890 sucks. It usually starts with a call saying the scan found something, followed by weeks or months of waiting through a follow-up scan, a specialist visit, and often a biopsy, with the possibility of cancer hanging over all of it. In a national survey of physicians, more than 99 percent said they had seen an incidental finding set off this kind of cascade, and most reported it had harmed patients financially, psychologically, or physically. Each workup also consumes a specialist slot and a pathologist’s time that someone with an actual problem then waits longer for. The harm can be physical, not only financial and emotional. A biopsy can bleed or get infected, and a suspicious spot on a kidney frequently goes to surgery, where 15 to 30 percent of the kidneys removed for a presumed tumor turn out to be benign. A number of those 890 healthy people end up losing part of an organ over something that posed no real threat.
This is how testing for anything rare behaves, and in people with no symptoms the thing you are testing for is usually rare. The clearest demonstration is the mammogram. When researchers give doctors the standard numbers and ask what a positive result means, most of them get it badly wrong and guess far too high. Give them the identical information as counts of actual people instead of percentages, and most of them get it right.
A symptom changes the prior. A scan ordered because something already hurts is checking a real suspicion, so a positive there carries weight. The same scan run on someone who feels fine is searching a population that is almost entirely healthy, where most of what turns up is the ordinary background of an aging body. That is why a doctor images you the moment you have a worrying symptom and resists when you just want to look, and why whole body MRI makes sense for a TP53 carrier and not for most people.
A low prior doesn’t automatically rule a test out. Every newborn in the country is screened for PKU, a metabolic disorder almost none of them have, because the confirmatory test is cheap, the treatment is a change in diet, and the thing it prevents is permanent brain damage. The calculation is always the false-positive rate times the cost of chasing a false alarm, set against how much earlier detection actually helps. For newborn PKU screening it is an easy call. For a whole body scan in a healthy adult, given where the accuracy and the follow-up systems are, it mostly isn’t, at least not yet.
The handoff
The handoff is everything that happens between the scan and the patient: the grading, the wording of the report, the decision about what comes next. The same probably-benign spot can move through handoff and end up as a note to recheck in a year or as a biopsy referral, depending on how it's graded and described.
Radiologists already use structured reporting systems that sort findings into tiers, so that something needing real attention and something worth a glance next year aren’t delivered with the same weight. A report can give the patient the actual probability that a finding is cancer instead of the word “abnormal,” though that is rarely done. And a finding can be watched over time rather than acted on right away, which matters because a spot that has been stable across three years of scans is a very different thing from a spot seen once, and the second and third scans are what let you tell them apart.
Over-reporting in wellness scans like Prenuvo is partly an economic artifact. When a scan costs a couple thousand dollars and you get one every few years, the company has every reason to report a full inventory of what it saw, because a long itemized list is how a single expensive scan justifies itself. Prenuvo lists the cyst on your kidney and the spot on your liver because that report is what you paid for. That incentive depends on scans being rare and expensive. Once they are cheap and frequent, the reason to surface every little thing weakens, and the natural thing to report is what changed since last time.
Guidelines for what to do with test results lag behind access to the test. The screening arrives first, and the rules for handling what it finds catch up later, usually after the harms pile up enough to force the issue. That catch-up is driven by the load those cases put on the health system: enough bad outcomes accumulate that the standards get rewritten. We have been through this cycle before, most clearly with PSA.
PSA detects a lot of cancer, much of it the slow kind that would never have killed the man who had it. The enthusiasm in the early 2000s for testing every man over fifty led to a wave of biopsies and surgeries, and to many men left incontinent or impotent after treatment for cancers that posed little real risk. In 2012 the US Preventive Services Task Force recommended against PSA screening outright.
But then in 2018 the Task Force moved back toward screening for men aged 55 to 69, as a shared decision rather than a blanket recommendation either way. What changed the recommendation later was not a new test. It was active surveillance, the practice of monitoring low-risk prostate cancer rather than operating on it right away, which went from unusual to standard over the following years. As the typical consequence of a positive result stopped being an unnecessary surgery, the balance of benefit and harm shifted.
In the six years after the 2012 recommendation to stop screening, the share of men first diagnosed with metastatic cancer rose.
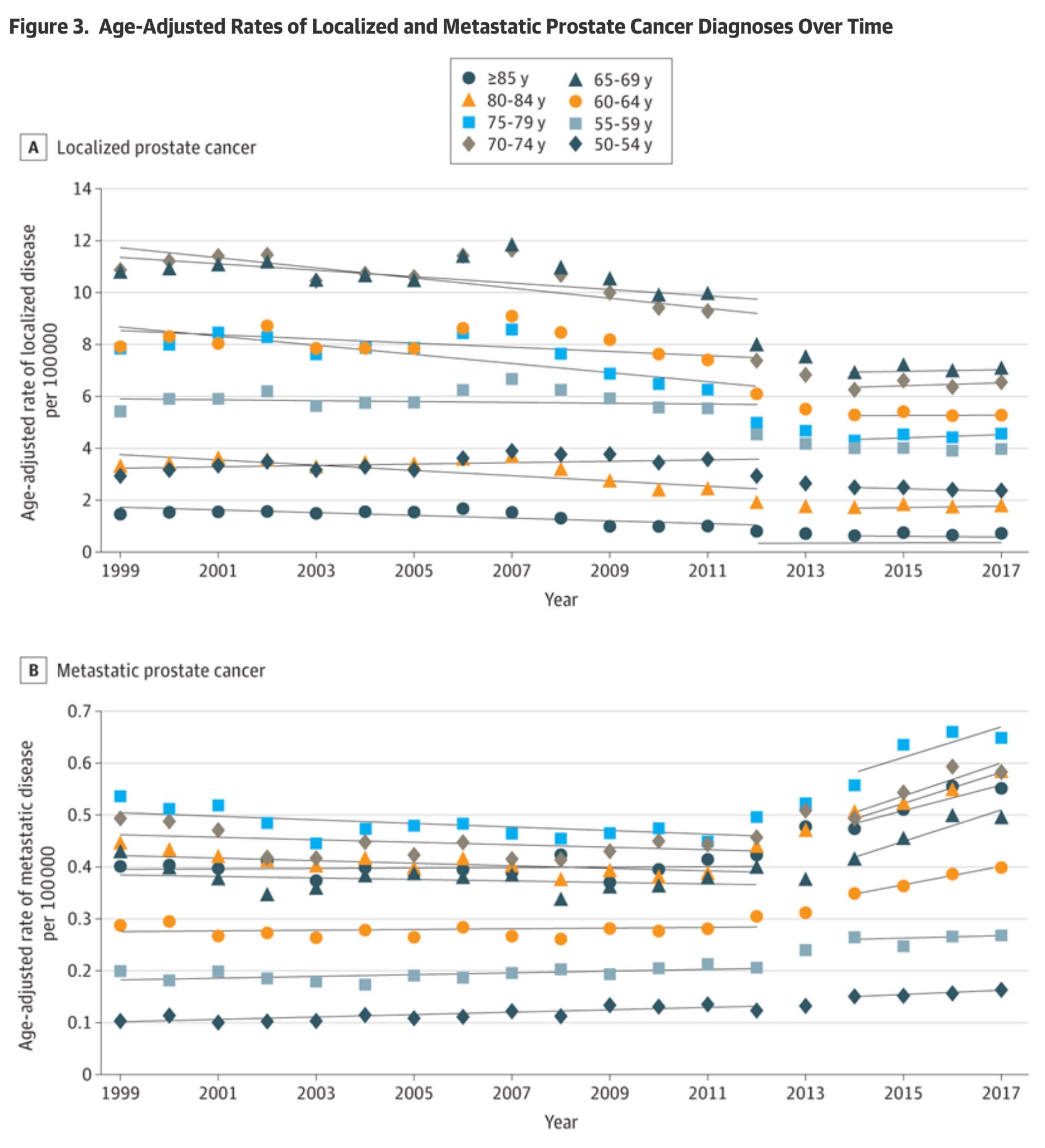
That whole correction depended on the cases landing inside the system, where the cost of getting it wrong eventually forced a fix. Cash-pay wellness scans sit outside that. They generate the findings and pass the cascade to a system they don’t answer to or pay for. The scans will get cheap before the rules catch up, and for a while the gap is going to land on people one kidney spot at a time.
What you call it
Say a man has the lowest grade of prostate cancer, the kind that essentially never spreads or kills, and the guidelines say to watch it rather than treat it. You can explain all of that to him, and he is still going to wake up most mornings knowing he has cancer.
The obvious question is whether you can just not tell him. But withholding a real diagnosis is a narrow and unfashionable idea in western medicine, and the direction of modern ethics is toward telling patients the truth and letting them decide what to do with it.
(I’ve always found it fascinating that in traditional Chinese medicine, patients are often not informed of a cancer diagnosis, although this practice has become less common recently.)
So the fight has moved somewhere stranger: whether the harmless thing should be called cancer in the first place. This has happened before. In 2016 a common low-risk thyroid tumor was reclassified and the word carcinoma was dropped from its name.
There is now a serious, unresolved push to do the same for the lowest grade of prostate cancer, renaming it something like “acinar neoplasm of low malignant potential,” so a person with a lesion that was never going to hurt them isn’t handed a cancer diagnosis and the years of fear that come with it. Pathologists are split, and one survey of them found about 82 percent against it. The thyroid version already went through.
Sharper signal
The scans will also get better, probably faster than the current debate assumes. False positives and overdiagnoses respond to better sensors, better software reading the images, and a growing record of what a given kind of spot turns into over years. The useful role for AI here is less about catching more and more about being confident enough to call a harmless finding harmless, so that fewer of them ever reach the patient as a scare. Repeat scanning does some of this on its own. Once there is a baseline, the question becomes whether a spot has changed rather than whether it looks dangerous, and that is both an easier question and a less frightening one to be asked. Collecting large longitudinal datasets now will let us build models that are better at categorizing risk.
There is a parallel in skin cancer screening. A dermatologist examining your whole skin for melanoma is doing roughly what a body scanner does, aimed at the one organ you can see, and it comes with the same overdiagnosis problem. US guidelines give routine skin checks for people without symptoms an insufficient-evidence rating, the same grade whole body MRI would get now. It is also one of the places AI has made the most progress at distinguishing a dangerous lesion from a harmless mole. There is little reason to expect the inside of the body to behave differently from the surface.
As the false-positive rate drops and the handling of each finding improves, the prior you need to justify scanning someone comes down with it. The line between the TP53 carrier who clearly should be scanned and the healthy adult who probably shouldn’t moves over time, toward more people reasonably being scanned and being hurt less often when they are.
More scanning is coming, and that’s good. Catching a cancer early in someone who feels fine is worth a lot, and these machines will do it for the kinds of cancer we usually find too late. After that, someone still has to tell the findings that matter from the ones that don't, and keep a harmless spot from becoming a diagnosis someone carries for years. But it’s a much better problem to have than not being able to see inside people at all.